

Approved Antibody Fragments and DMPK Strategies: Fab, scFv, and VHH
-

Articles
-

Dec 11, 2025
Antibody Therapy represents a targeted treatment modality that utilizes antibody-based molecules to treat diseases. Monoclonal antibodies (mAbs) are immunoglobulins secreted by plasma B cells in response to specific antigens. Antibodies fulfill diverse roles within the human immune system, including the facilitation of humoral and cellular immune responses to diverse antigens, characterized by high specificity and long-lasting efficacy. Since the FDA approval of the first monoclonal antibody, Muromonab-CD3, in 1986, antibodies have become a prominent class of therapeutic drugs. To date, over 200 antibody therapies have been approved globally [1], encompassing indications such as oncology, immune-related disorders, infectious diseases, and hematological conditions. The advantage of antibody therapy lies in its high selectivity and high affinity for targets. Over the past four decades, the development paradigm for antibody-based drugs has evolved rapidly, expanding from traditional monoclonal antibodies to various formats such as antibody-drug conjugates (ADCs), bispecific/multispecific antibodies, and antibody fragments [2]. This article primarily introduces the progress in antibody fragment drugs, including antigen-binding fragments (Fabs), single-chain variable fragment (scFv) constructs, and heavy-chain variable fragment (VHH, nanobody), and their pharmacokinetic characteristics.
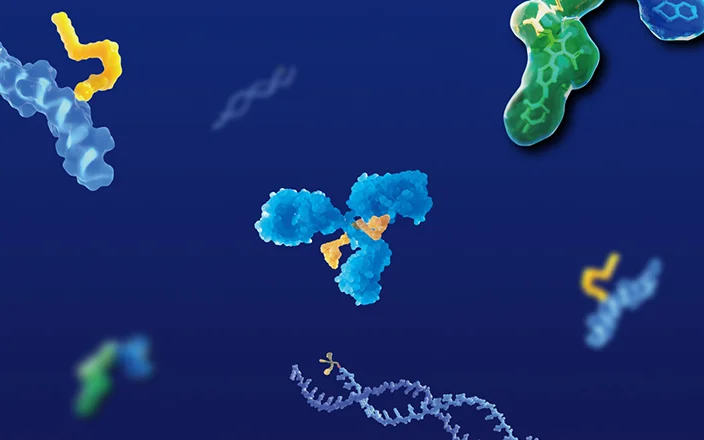
, antibody-drug conjugate (b), bispecific antibody (c), and antibody fragments (d). Fragments include antigen-binding fragments (Fabs), single-chain variable fragment (scFv) constructs, and domain antibodies")
Figure 1. Antibody formats: Typical antibody (a), antibody-drug conjugate (b), bispecific antibody (c), and antibody fragments (d). Fragments include antigen-binding fragments (Fabs), single-chain variable fragment (scFv) constructs, and domain antibodies. [2]
What Are Antibody Fragments and Their Types
Antibody molecules can be processed by biochemical or genetic means to isolate individual domains. These individual domain-derived antibody fragment drugs can be classified into three principal categories: Antigen-binding fragments (Fab), Single-chain variable fragments (scFv), and Heavy-chain variable fragments (VHH, nanobody). Approved antibody fragments are listed in Table 1 [1, 3]. An introduction to each antibody fragment type is provided below.
Antigen-Binding Fragment (Fab)
By enzymatically cleaving the heavy chain above the hinge region with papain, an antibody can be digested into the Fc fragment (crystallizable fragment) and two Fab fragments. The Fab fragment has a molecular weight of approximately 50 kDa, only about one-third that of a full-length antibody, which confers improved tissue penetration. Furthermore, Fab fragments lack the Fc region, and therefore do not mediate effector functions such as antibody-dependent cellular cytotoxicity (ADCC), antibody-dependent cellular phagocytosis (ADCP), or complement-dependent cytotoxicity (CDC), resulting in a markedly shorter in vivo half-life. Fab fragments represent the earliest monoclonal antibody (mAb) fragment therapeutics, and to date, the FDA has approved four drugs by 2025: Abciximab, Ranibizumab, Certolizumab Pegol, and Idarucizumab, as shown in Table 1.
Single-Chain Variable Fragment (scFv)
Single-chain variable fragments (scFvs) are recombinant molecules in which the variable regions of the light and heavy immunoglobulin chains, responsible for antigen binding, are engineered into a single polypeptide. Typically, the VH and VL sequences are connected by a flexible linker. This configuration enables the generation of variants to optimize binding affinity and stability [4]. Diverse scFv molecules can form bivalent structures through complementary region pairing, exist as single chains with tandem scFvs, or form bispecific tandem scFvs (bis-scFvs) [4]. Four scFv-based drugs have received FDA approval by 2025. Blinatumomab, a bispecific tandem scFv targeting CD19 and CD3, was approved in 2014 for the treatment of acute lymphoblastic leukemia. Moxetumomab pasudotox, an immunotoxin targeting human CD22, was approved in 2018 for the treatment of hairy cell leukemia. Brolucizumab, a humanized scFv that inhibits VEGF-A, was approved in 2019 for the treatment of neovascular age-related macular degeneration. Tebentafusp, a novel T cell receptor (TCR) bispecific immunotherapy comprising a soluble TCR fused to an anti-CD3 immune effector domain, was approved in 2022 for the treatment of metastatic uveal melanoma.
Table 1. Approved Antibody Fragments
Fragment Type | Generic Name | Brand Name | Target | Molecular Weight (kDa) | First Approved Indication | Dosing Route | First Approval | Company |
Fab | Abciximab | Reopro | GPIIb/IIIa | 48 | Prevention of thrombosis during angioplasty | IV | US, 1994 | Jassen |
Fab | Ranibizumab | Lucentis | VEGF-A | 48 | Macular degeneration | IVT | US, 2006 | Genentech |
PEGylated Fab | Certolizumab Pegol | Cimzia | TNF | 90 | Crohn's disease | IV | US, 2008 | UCB Pharma |
Fab | Idarucizumab | Praxbind | Dabigatran | 48 | Reversal of dabigatran-induced anticoagulation | IV | US, 2015 | Boehringer Ingelheim |
Tandem scFv | Blinatumomab | Blincyto | CD19/CD3 | 55 | Acute lymphoblastic leukemia | IV | US, 2014 | Amgen |
dsFv Immunotoxin | Moxetumomab Pasudotox | Lumoxiti | CD22 | 63 | Hairy cell leukemia | IV | US, 2018 | AstraZeneca |
scFv | Brolucizumab | Beovu | VEGF-A | 26 | Neovascular (wet) age-related macular degeneration | IVT | US, 2019 | Novartis Pharmaceuticals |
scFv-TCR Fusion Protein | Tebentafusp | Kimmtrak | gp100, CD3 | 76 | Metastatic uveal melanoma | IV | US, 2022 | Immunocore Ltd |
VHH (bivalent) | Caplacizumab | Cablivi | von Willebrand factor | 28 | Acquired thrombotic thrombocytopenic purpura | IV-SC | EU, 2018 | Sanofi |
VHH-Fc | Envafolimab | Endvida | PD-L1 | 80 | Recurrent advanced solid tumors | SC | China, 2021 | 3D Medicines & Alphamab Co. Ltd & Simcere |
VHH (trivalent) | Ozoralizumab | Nanozora | TNF, Albumin | 38 | Rheumatoid arthritis | SC | Japan, 2022 | Taisho Pharmaceutical (Sanofi) |
Heavy-Chain Variable Fragment (VHH, Nanobody)
There are heavy-chain antibodies naturally lacking light chains in camels. By cloning their variable region, single-domain antibodies could be obtained, which are composed solely of the heavy-chain variable region, known as VHH (variable domain of heavy chain antibody), also referred to as nanobodies (Nb). These represent the smallest functional antigen-binding fragments [5].
VHH shares the same domain structure as the VH domain of conventional IgG antibodies (Figure 2), comprising conserved framework regions (FR1, FR2, FR3, FR4) and complementarity-determining regions (CDR1, CDR2, CDR3). The VH domain contains four highly conserved hydrophobic amino acids in FR2 (V37, G44, L45, W47). In contrast, VHH replaces these residues with hydrophilic amino acids (F37, E45, R47, G52), thereby enhancing solubility. Additionally, the CDR1 and CDR3 in VHH are frequently connected by an interloop disulfide bond, improving structural stability. Furthermore, the average lengths of CDR1 and CDR3 in VHH are slightly longer than those in VH. The flexible CDR3 loop of VHH acts like a slender "finger", enabling access to cryptic epitopes and cavities on target antigens that are inaccessible to conventional antibodies, thus achieving superior functional activity [5].
 Conventional IgG antibody consists of two identical heavy chains, composed of VH, CH1, CH2, and CH3 domains, and two identical light chains, composed of VL and CL domains. Camelid heavy-chain antibody contains one VHH domain and two constant regions (CH2 and CH3). (B) Differences in amino acid sequences between VH and VHH, and the folded structures of the VH and VHH domains")
Figure 2. (A) Conventional IgG antibody consists of two identical heavy chains, composed of VH, CH1, CH2, and CH3 domains, and two identical light chains, composed of VL and CL domains. Camelid heavy-chain antibody contains one VHH domain and two constant regions (CH2 and CH3). (B) Differences in amino acid sequences between VH and VHH, and the folded structures of the VH and VHH domains. [5]
VHH offers several advantages, including efficient tissue penetration, high stability, tolerance to extreme conditions, and high solubility. VHH demonstrates prolonged stability at 4 °C and -20 °C, tolerates high temperatures (60-80 °C) and proteolysis, withstands non-physiological pH (3.0-9.0), and resists high pressure (500-750 MPa). Compared to conventional antibodies (molecular weight ~150 kDa), VHH, as the smallest antibody fragment (molecular weight ~15 kDa), exhibits superior tissue penetration, allowing it to reach diseased sites inaccessible to conventional antibodies. Moreover, nanobodies can effectively traverse the blood-brain barrier, offering a new approach for central nervous system drug delivery. However, due to their small size, nanobodies are rapidly cleared by renal excretion, resulting in a short half-life. While this avoids potential toxic effects, it may also limit sustained therapeutic efficacy. Strategies to extend half-life include PEGylation, conjugation, or fusion with albumin and fusion with the antibody Fc region. Additionally, VHH shares high sequence similarity (approximately 75-90%) with human VH, resulting in low immunogenicity. By 2025, three VHH-based drugs will have been approved globally: the bivalent VHH drug Caplacizumab (FDA approval, 2018), the VHH-Fc fusion protein Envafolimab (China approval, 2021), and the trivalent VHH drug Ozoralizumab (Japan approval, 2022), as listed in Table 1.
Antibody Fragments vs. Monoclonal Antibodies
Compared to monoclonal antibodies, antibody fragment drugs possess distinct benefits and drawbacks. Table 2 summarizes the comparison of advantages and disadvantages between various antibody fragment drugs and monoclonal antibodies [6]. Due to the absence of an Fc segment, antibody fragment drugs exhibit a significantly shorter in vivo half-life compared to full-length antibodies, but demonstrate enhanced tissue penetration. Additionally, antibody fragments show advantages in aspects like water solubility and stability.
Table 2. A Comparison between monoclonal antibody, Fab, scFv, and nanobody in properties [6]
Property | Monoclonal Antibody | Fab | scFv | VHH |
Molecular Weight | 150 kDa | ~50 kDa | 30-35 kDa | 12-15 kDa |
Molecular Size (Diameter × Length) | 10-15 × 10 nm | 15.9 × 0.95 nm | 2 × 3 nm | 1 × 2.5 nm |
Half-Life in Blood | Days to weeks | 7.2-19.2 h | < 1 h | < 1 h |
Preferred Expression System | Mammalian cells | Bacteria | Bacteria | Yeast |
Water Solubility | + | + | + | +++ |
Aggregation | +++ | ++ | ++ | + |
Stability under Harsh Conditions | ++ | ++ | + | +++ |
Tissue Penetration | + | + | ++ | +++ |
Paratope diversity | + | + | ++ | +++ |
Affinity | ++ | ++ | ++ | ++ |
Complexity of library construction techniques | +++ | +++ | ++ | + |
Ease of Expression | + | + | + | +++ |
DMPK Strategies for Antibody Fragments
Similar to antibody drugs, the DMPK requirement for the regulatory submission of antibody fragment drugs primarily includes in vivo pharmacokinetics (PK) data. When designing PK studies for antibody fragment drugs, key considerations include: 1) The intrinsic properties of the drug; 2) The intended indication of the drug. The nonclinical PK studies submitted in support of approved antibody fragment drugs are summarized in Table 3.
Both Ranibizumab and Brolucizumab target VEGF-A, and their indications are ocular diseases. In their respective FDA submissions, both provided pharmacokinetic data about intravitreal (IVT) administration in monkeys and rabbits. Following IVT administration, the vitreous humor, aqueous humor, various retinal layers, other ocular tissues (e.g., the ciliary body, iris, corneal endothelium), and serum samples should be collected to monitor drug concentrations and anti-drug antibody (ADA) responses.
Tebentafusp is a novel bispecific protein composed of a soluble TCR fused to an anti-CD3 immune effector domain: one terminus is a high-affinity soluble T-cell receptor that binds a specific antigen, and the other terminus is an immune effector domain recognizing CD3. It targets gp100. Due to its specificity for a human HLA-presented gp100 peptide and the lack of suitable conventional animal models, pharmacokinetic evaluations were conducted exclusively in mice.
Compared to antibody drugs, antibody fragment drugs have lower molecular weights and superior tissue penetration. Therefore, in some cases, it is necessary to investigate the tissue distribution of antibody fragment drugs. Certolizumab Pegol is a conjugation of a 50 kDa humanized IgG Fab' fragment to a 40 kDa polyethylene glycol (PEG) moiety. Caplacizumab consists of 259 amino acids, formed by linking two 128-amino-acid humanized nanobodies against vWF (von Willebrand factor) via an AAA linker (composed of three alanines), with a molecular weight below 28 kDa. In their FDA submission materials, in addition to conventional in vivo serum PK, tissue distribution studies using 125I-labeled radioisotopes were carried out for both drugs. Furthermore, Idarucizumab and Caplacizumab conducted urinary excretion studies in animal models.
For antibody fragment drugs, commonly used analytical methods include enzyme-linked immunosorbent assay (ELISA), liquid chromatography-tandem mass spectrometry (LC-MS/MS), and Western Blot. WuXi AppTec DMPK offers a variety of detection methods, including ELISA, MSD electrochemiluminescence, Hybrid LBA-LC-MS, and Universal Sensitive Competitive ELISA (USCE), specifically designed for quantifying antibody fragment drugs lacking conserved regions.
Table 3. Overview of Nonclinical Pharmacokinetic Studies for Approved Antibody Fragments [3]
Fragment Type | Generic Name | DMPK Study Design | Analytical Method | ||
Plasma/Serum PK study design | Tissue Distribution Study Design | Excretion | |||
Fab | Ranibizumab | 1. IVT administration in rabbits to detect drug concentration in serum; | 1. ITV/SCJ/IC administration in rabbits to detect drug concentration in retinal & serum; | / | ELISA |
PEGylated Fab | Certolizumab Pegol | 1. IV infusion of 125I-labeled drug in monkeys to detect blood radioactivity; | IV administration of 125I-labeled drug in rats to detect, radioactive concentration in blood & tissues. | / | ELISA |
Fab | Idarucizumab | 1. IV administration in rats to detect drug concentration in blood; | / | 1. IV administration of the drug in rats to evaluate urinary excretion; | ELISA LC-MS/MS |
scFv (Tandem) | Blinatumomab | 1. Repeat IV administration in mice TK to detect drug concentration in blood. | / | / | |
scFv (dsFv Immunotoxin) | Moxetumomab Pasudotox | 1. Repeat IV administration in rats to detect drug concentration in blood; | / | / | ELISA |
scFv | Brolucizumab | 1. IVT administration in rabbits to detect drug concentration in serum; | 1. IVT administration in rabbits to detect drug concentration in ocular tissues and serum; | / | ELISA |
scFv-TCR Fusion | Tebentafusp | Single/repeat IV administration in mice to detect drug concentration in blood. | / | / | |
VHH (bivalent) | Caplacizumab | Single/multiple SC/IM administration in Guinea pigs to detect drug concentration in blood. | IV administration of 125I-labeled drugs in mice to detect radioactive concentration in blood & tissues. | IV administration of the drug in monkeys to detect the drug concentration in urine. | Western Blot, ELISA |
Conclusion and Future Perspectives
Compared to full-length antibodies, antibody fragments demonstrate considerable promise in both therapeutic and diagnostic applications, owing to attributes such as excellent tissue penetration and low immunogenicity. VHH, in particular, exhibits exceptional stability, high solubility, and favorable tissue penetration. Bispecific antibodies constructed from VHH have become a focal point of research. For example, SOR102, developed by Sorriso Pharmaceuticals, is an oral VHH bispecific antibody targeting both TNF-α and IL-23p19; Genentech has also reported related oral VHH drugs [7]. Furthermore, LQ036 and LQ043H, VHH-based inhalation drugs developed by Novamab, are undergoing clinical trials. FL801, a radioligand conjugate drug developed by Full-Life Technologies based on VHH, shows promising anti-tumor activity with low renal accumulation. These recent advancements are summarized in Table 4.
In recent years, antibody fragment drugs have demonstrated tremendous potential in drug discovery and development based on their inherent advantages. They facilitate diverse administration routes, such as oral and inhaled delivery, and enable targeting of disease areas that are challenging for conventional antibodies, thereby driving the application of antibodies towards broader and more precise clinical indications, becoming a significant impetus for innovation in antibody therapeutics. The rapid advancement of antibody fragment drugs has substantially elevated the demand for associated testing services and imposed more stringent requirements on testing standards. WuXi AppTec DMPK is dedicated to expediting innovation and consistently develops specialized solutions for the antibody fragment services, with the objective of further facilitating their clinical translation.
Table 4. Recent Case Studies in Antibody Fragment Drug Development
Drug Format | Component Fragment | Representative Drug (Target) | Route of Administration | Disease Area | Current Stage |
Bispecific/Multispecific Antibody | VHH | SOR102 (TNF-α/IL-23p19) | Oral | Crohn's Disease | Phase I |
Bivalent Nanobody | VHH | LQ036 (IL-4Rα) | Inhalation | Respiratory Diseases | Phase I |
Bivalent Nanobody | VHH | LQ043H (TSLP) | Inhalation | Respiratory Diseases | Phase II |
Radioligand Conjugate | Radionuclide-VHH | FL801 (B7-H3) | Intravenous Injection | Cancer | Preclinical |
Authors: Xueyi Lu, Qigan Cheng, Jing Jin
Talk to a WuXi AppTec expert today to get the support you need to achieve your drug development goals.
Committed to accelerating drug discovery and development, we offer a full range of discovery screening, preclinical development, clinical drug metabolism, and pharmacokinetic (DMPK) platforms and services. With research facilities in the United States (New Jersey) and China (Shanghai, Suzhou, Nanjing, and Nantong), 1,000+ scientists, and over fifteen years of experience in Investigational New Drug (IND) application, our DMPK team at WuXi AppTec are serving 1,600+ global clients, and have successfully supported 1,700+ IND applications.
Reference
[1] http://www.antibodysociety.org/resources.
[2] Mullard A. FDA approves 100th monoclonal antibody product. Nat Rev Drug Discov. 2021;20(7):491-495. doi:10.1038/d41573-021-00079-7
[3] http://www.fda.gov
[4] Nelson AL. Antibody fragments: hope and hype. MAbs. 2010;2(1):77-83. doi:10.4161/mabs.2.1.10786
[5] Muyldermans S, Baral TN, Retamozzo VC, De Baetselier P, De Genst E, Kinne J, Leonhardt H, Magez S, Nguyen VK, Revets H, Rothbauer U, Stijlemans B, Tillib S, Wernery U, Wyns L, Hassanzadeh-Ghassabeh G, Saerens D. Camelid immunoglobulins and nanobody technology. Vet Immunol Immunopathol. 2009 Mar 15;128(1-3):178-83.
[6] Liu L, Tu B, Sun Y, Liao L, Lu X, Liu E, Huang Y. Nanobody-based drug delivery systems for cancer therapy. J Control Release. 2025 May 10;381:113562.
[7] Ota N, Davies CW, Kang J, Yan D, Scherl A, Wong A, Cook R, Tao X, Dunlap D, Klabunde S, Mantik P, Mohanan V, Lin W, McBride J, Sadekar S, Storek KM, Lupardus P, Ye Z, Ackerly Wallweber H, Kiefer JR, Xu M, Chan P, Nagapudi K, Yi T, Koerber JT. Engineering a protease-stable, oral single-domain antibody to inhibit IL-23 signaling. Proc Natl Acad Sci U S A. 2025 Jun 3;122(22):e2501635122.










Related Services and Platforms



Stay Connected
Keep up with the latest news and insights.

